
Psychiatric diagnosis is the clinical process by which a trained clinician identifies a specific mental health condition based on symptom patterns, distress, and measurable impairment in daily functioning. The formal framework for this process comes from two major diagnostic manuals: the DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision) and the ICD-11 (International Classification of Diseases). Understanding psychiatric diagnosis matters because a clear, accurate diagnosis is the foundation of any effective treatment plan. Without it, care becomes guesswork. With it, you and your clinician can move forward with purpose.
What does understanding psychiatric diagnosis actually involve?
A psychiatric diagnosis is not a label stamped on a person. It is a clinical hypothesis. Clinicians use it to organize what they observe, guide treatment decisions, and communicate clearly with other providers. The DSM-5-TR requires that symptoms cause significant distress or impairment in social, occupational, or daily functioning before a diagnosis applies. That threshold matters. It separates a mental disorder from ordinary stress, grief, or a rough patch in life.
The two primary diagnostic systems, DSM-5-TR and ICD-11, serve different purposes. DSM-5-TR is used most widely in the United States for clinical practice, research, and insurance documentation. ICD-11 is the World Health Organization’s global standard, used broadly in international health settings. Both systems share the core principle that symptoms alone are not enough. Context, duration, and functional impact all factor into the picture.

We often tell patients that a diagnosis is a starting point, not a destination. It gives your care a direction. It does not define who you are.
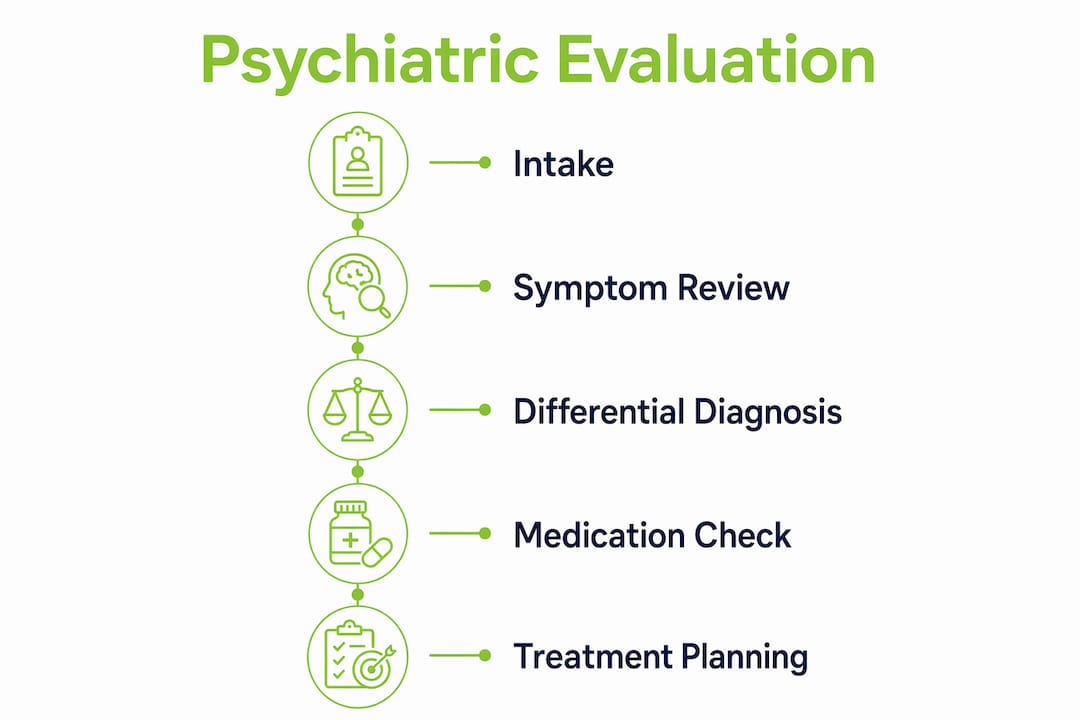
How is a psychiatric evaluation conducted?
The psychiatric assessment process follows a structured sequence. Initial psychiatric evaluations typically last 45–60 minutes and cover symptoms, medical history, family psychiatric history, and lifestyle factors. That time goes fast. Clinicians use structured clinical interviews alongside standardized rating scales to build a quantitative picture of what you are experiencing.
Here is what a standard evaluation covers:
- Current symptoms: What you are feeling, how long it has been happening, and how severe it is
- Medical history: Past diagnoses, surgeries, chronic conditions, and current medications
- Family history: Psychiatric conditions in first-degree relatives, which can signal genetic risk
- Lifestyle factors: Sleep patterns, exercise, diet, substance use, and major life stressors
- Functional impact: How symptoms affect your work, relationships, and daily routines
Screening questionnaires and direct questions about symptom timing and severity are standard. After gathering this information, the clinician explains their working diagnosis, outlines treatment options, and describes next steps clearly.
Differential diagnosis is a critical part of this process. Before confirming any psychiatric disorder, clinicians follow a structured sequence that rules out medical conditions, substance use, and medication side effects as possible causes. Thyroid disorders, for example, can mimic depression or anxiety closely. A clinician who skips this step risks misdiagnosis and ineffective treatment.
Pro Tip: Bring a written list of every medication, supplement, and substance you use regularly. Clinicians must rule out medication-related causes before assigning a psychiatric diagnosis, and this list saves time and prevents errors.
What does a psychiatric diagnosis mean for your treatment?
A diagnosis gives your treatment plan a framework. It tells your clinician which therapies have the strongest evidence, which medications are most likely to help, and what lifestyle changes may reduce symptoms. Treatment is personalized and depends on your unique history, preferences, and goals. Medication is not automatically prescribed at every evaluation.
Patients often worry that receiving a diagnosis means they are broken or permanently defined by a condition. That concern is understandable. But a diagnosis is better understood as a clinical tool. It creates a shared language between you and your care team. It also opens doors to resources, accommodations, and treatments that would otherwise be inaccessible.
“A psychiatric diagnosis is not a verdict. It is a map. It tells you where you are so you can figure out where you want to go. The map can be revised as you learn more about yourself and as your symptoms change over time.”
Not every patient receives a definitive diagnosis at the first visit. Ongoing assessment is sometimes necessary, particularly when symptoms overlap across multiple conditions or when the clinical picture is still developing. That uncertainty is normal. It reflects the honest complexity of mental health, not a failure of the process.
Here is what a diagnosis can guide:
- Therapy selection: Cognitive Behavioral Therapy (CBT) for depression and anxiety, Dialectical Behavior Therapy (DBT) for emotional dysregulation, and other evidence-based approaches
- Medication decisions: Antidepressants, mood stabilizers, stimulants, or antipsychotics, depending on the condition
- Lifestyle recommendations: Sleep hygiene, exercise protocols, and stress reduction strategies tailored to your diagnosis
- Referrals and support: Connections to specialists, support groups, or music therapy programs that complement clinical care
What are the thresholds and criteria for a psychiatric diagnosis?
The threshold for any psychiatric diagnosis rests on two pillars: clinically significant distress and functional decline. The DSM-5-TR standard distinguishes mental disorders from normal life stress by requiring that symptoms meaningfully impair how a person functions. Feeling sad after a loss is human. Feeling unable to work, maintain relationships, or care for yourself for weeks on end is clinically significant.
A useful framework for understanding what qualifies as a mental disorder is the 5 D’s of psychological disorders:
- Deviance: Thoughts, feelings, or behaviors that fall outside cultural norms
- Distress: Significant personal suffering caused by the symptoms
- Dysfunction: Impairment in social, occupational, or daily functioning
- Duration: Symptoms that persist beyond a brief or situational timeframe
- Danger: Risk of harm to oneself or others
The table below shows how common psychiatric diagnoses map to these criteria:
| Diagnosis | Core Symptom Pattern | Minimum Duration |
|---|---|---|
| Major depressive disorder | Persistent low mood, loss of interest, fatigue | 2 weeks |
| Bipolar disorder | Alternating depressive and manic episodes | Varies by episode type |
| Generalized anxiety disorder | Excessive worry, physical tension, restlessness | 6 months |
| Schizophrenia | Hallucinations, delusions, disorganized thinking | 6 months |
| ADHD | Inattention, hyperactivity, impulsivity across settings | 6 months |
Medical causes and substance use are always ruled out first. A patient presenting with anxiety symptoms who drinks heavily every night may be experiencing alcohol withdrawal, not generalized anxiety disorder. Getting this sequence right is what makes differential diagnosis so central to accurate care.
How can you prepare for your psychiatric evaluation?
Preparation makes a real difference. Patients who prepare a list of 3–5 specific concerns before their appointment help clinicians tailor the evaluation and build a stronger foundation for care. The evaluation session is limited. Arriving organized means more of that time goes toward understanding your situation rather than gathering basic facts.
Practical steps to take before your appointment:
- Write down your 3–5 most pressing symptoms or concerns, including when they started
- Bring a complete list of current medications, supplements, and any substances you use
- Gather your medical history, including past diagnoses and any relevant lab results
- Note any family history of depression, anxiety, bipolar disorder, ADHD, or other conditions
- Think about how your symptoms affect your work, relationships, and daily routines
During the appointment, ask clear questions. Ask what the working diagnosis is and why. Ask what treatment options exist and what the evidence says about each. Ask about medication risks and what to expect in the weeks ahead. The first psychiatric appointment is a collaborative partnership designed to understand your unique story, biology, and environment. You are not a passive recipient of a label. You are an active participant in building a care plan.
Pro Tip: After your appointment, write down the working diagnosis and the agreed next steps while the details are fresh. Patients who track this information engage more effectively with their personalized treatment plan over time.
Key Takeaways
A psychiatric diagnosis is a clinical tool grounded in DSM-5-TR criteria, requiring both symptom presence and meaningful functional impairment before any condition is formally identified.
| Point | Details |
|---|---|
| Diagnosis requires impairment | Symptoms must cause real distress or functional decline, not just discomfort. |
| Evaluation is structured | A 45–60 minute clinical interview covers symptoms, history, and lifestyle factors. |
| Differential diagnosis comes first | Medical causes and substance use are ruled out before any psychiatric label is assigned. |
| Diagnosis guides treatment | It determines therapy type, medication options, and lifestyle recommendations. |
| Preparation improves outcomes | Bringing a list of 3–5 concerns and a full medication list makes the evaluation more effective. |
What I have learned after years of doing this work
The patients who get the most out of their diagnostic evaluation are almost always the ones who come prepared and willing to be honest. Not perfectly articulate. Not medically trained. Just honest. That combination of preparation and candor gives us far more to work with than any questionnaire alone.
What I have also noticed is that many patients arrive carrying a fear that a diagnosis will reduce them to a category. That fear is worth naming directly. A diagnosis does not shrink a person. It gives us a shared vocabulary to work with. I have seen patients feel genuine relief when a diagnosis finally explains years of confusion. That relief is not resignation. It is clarity.
Diagnostic uncertainty is also real, and we should say so more often. Mental health conditions overlap. Symptoms evolve. A working diagnosis at the first visit may shift as we learn more. That is not a failure of psychiatry. It is psychiatry being honest about complexity. The goal is always to get closer to the truth, not to be right on the first try.
If you are preparing for your first evaluation, or wondering whether to seek one, the reasons to seek psychiatric care are worth reading before you go. Knowing why you are there makes the conversation more productive from the start.
— Felix
Nortexpsychiatry offers structured evaluations built around your needs
At Nortexpsychiatry, psychiatric evaluations follow DSM-5-TR standards and are designed to give you a clear picture of what is happening and why. We serve patients across Allen, Frisco, McKinney, Plano, and the broader North Dallas area, with both in-person and telehealth options available. Our approach combines a thorough clinical interview with personalized, evidence-based treatment planning. Whether you are seeking answers about anxiety, depression, ADHD, or a mood disorder, we work with you to build a care plan that fits your life. Learn more about what to expect from a structured psychiatric evaluation and take the first step toward clarity.
FAQ
What is a psychiatric diagnosis?
A psychiatric diagnosis is a clinician’s formal identification of a mental health condition based on symptom patterns, duration, and functional impairment assessed against DSM-5-TR or ICD-11 criteria. It serves as the foundation for building an effective, personalized treatment plan.
How long does a psychiatric evaluation take?
Initial psychiatric evaluations typically last 45–60 minutes and cover symptoms, medical and family history, lifestyle factors, and standardized rating scales. Some complex cases require follow-up sessions before a working diagnosis is confirmed.
Can I receive a diagnosis at my first appointment?
Many patients receive a working diagnosis at their first visit, but not always. Overlapping symptoms or incomplete history may require additional sessions before a clinician can assign a diagnosis with confidence.
What is the difference between DSM-5-TR and ICD-11?
DSM-5-TR is the primary diagnostic standard used in the United States for clinical practice and insurance documentation. ICD-11 is the World Health Organization’s global classification system, used more broadly in international health settings.
Does a psychiatric diagnosis mean I will be on medication?
Not automatically. Treatment depends on your unique diagnosis, history, and preferences, and may involve therapy, lifestyle changes, medication, or a combination of all three.



