
Cognitive behavioral therapy (CBT) is a structured, time-limited form of talk therapy that targets the connection between your thoughts, emotions, and behaviors to reduce psychological distress. Most CBT programs run for 12 to 16 weekly sessions, each lasting about 50 minutes. The approach is grounded in a straightforward idea: the way you interpret events shapes how you feel and what you do. By changing those interpretations, you can change your emotional responses. CBT is the most widely researched psychotherapy in the world, with strong clinical evidence for anxiety, depression, PTSD, and OCD.
What is cognitive behavioral therapy and how does it work?
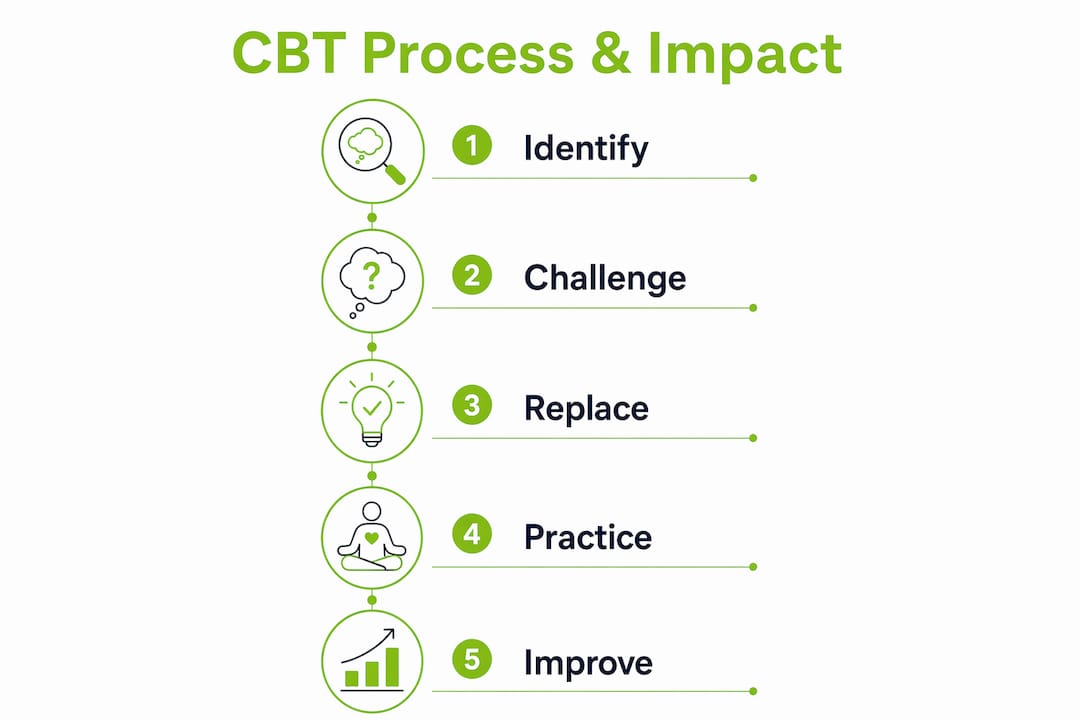
CBT works by teaching you to notice automatic thoughts, test whether they are accurate, and replace distorted ones with more realistic alternatives. This process is called cognitive restructuring. It is not about thinking positively. It is about thinking accurately.
The therapy operates on a simple model. A situation triggers a thought. That thought produces an emotion. That emotion drives a behavior. CBT intervenes at the thought level, which is where the most durable change happens.
Three core techniques define how CBT achieves that change:
- Cognitive restructuring. You and your therapist examine the evidence for and against a distressing automatic thought. For example, if you believe “everyone at the party thinks I am boring,” you test that belief against actual facts rather than accepting it as true.
- Behavioral activation. For depression especially, CBT uses scheduled activities to break the cycle of withdrawal and low mood. Doing more leads to feeling more, not the other way around.
- Gradual exposure. For anxiety and phobias, you face feared situations in a controlled, step-by-step way. Each successful exposure reduces the fear response over time.
Homework is not optional in CBT. Between-session practice is where most of the real learning happens. Your therapist assigns logs, thought records, or behavioral experiments to complete before the next session. Skipping homework slows progress significantly.
Pro Tip: Keep a thought record on your phone between sessions. Writing down the situation, your automatic thought, and the emotion it triggered takes two minutes and gives your therapist concrete material to work with.
CBT also stays focused on present problems. It does not spend sessions excavating your childhood or analyzing unconscious conflicts. That present focus keeps therapy goal-directed and time-limited, which many patients find more manageable.
Is cognitive behavioral therapy effective? What the research shows
CBT is effective. That is not a marketing claim. It is the conclusion of meta-analyses published in JAMA Psychiatry covering thousands of patients across multiple conditions.
The research shows large effect sizes for major depression, panic disorder, social anxiety, generalized anxiety disorder, bulimia, binge eating disorder, and OCD. Effect sizes for PTSD and specific phobias are even larger. Effect size matters because it tells you how meaningful the improvement is, not just whether it is statistically detectable.
| Condition | Evidence level | CBT status |
|---|---|---|
| Major depression | Meta-analyses, RCTs | First-line treatment |
| Generalized anxiety disorder | Meta-analyses, RCTs | First-line treatment |
| PTSD | Meta-analyses, RCTs | Very large effect size |
| OCD | Meta-analyses, RCTs | First-line treatment |
| Specific phobias | Meta-analyses, RCTs | Very large effect size |
| Panic disorder | Meta-analyses, RCTs | Large effect size |
For moderate-to-severe depression and panic disorders, combining CBT with medication produces better outcomes than either treatment alone. That combination approach is worth discussing with a psychiatrist if your symptoms are significant. You can read more about how psychiatric care benefits anxiety and depression to understand what that looks like in practice.
CBT’s structured format also makes it easier to measure progress. Sessions follow a consistent pattern, goals are set early, and outcomes are tracked. That accountability is part of why it works.
How does CBT compare to other types of therapy?
CBT is problem-focused and present-oriented. That makes it distinctly different from several other common approaches. CBT targets current thoughts and behaviors rather than exploring unconscious childhood roots, which is the territory of psychodynamic therapy.
| Therapy type | Time frame | Focus | Structure |
|---|---|---|---|
| Cognitive behavioral therapy | 12–20 sessions | Present thoughts and behaviors | Highly structured, agenda-driven |
| Psychodynamic therapy | Months to years | Unconscious patterns, past relationships | Less structured, exploratory |
| Humanistic therapy | Variable | Self-actualization, personal growth | Flexible, client-led |
| Behavior therapy | Variable | Behaviors only, not cognitions | Structured, exposure-based |
| Integrative therapy | Variable | Combines multiple approaches | Varies by therapist |
Psychodynamic therapy can produce lasting change, but it takes longer and suits patients who want to understand the deeper roots of their patterns. CBT suits patients who want to address a specific problem within a defined timeframe. Neither is universally superior. The right fit depends on what you are dealing with and what you are ready to do.
For anxiety specifically, CBT’s exposure component gives it an edge over purely talk-based approaches. You can learn more about how anxiety treatment works step by step to see where CBT fits into a broader care plan.
What to expect in cognitive behavioral therapy sessions
A typical CBT session follows a predictable structure. That predictability is intentional. It keeps sessions efficient and focused.
- Mood check. Your therapist asks how you have been feeling since the last session, often using a brief rating scale.
- Agenda setting. You and your therapist agree on what to address in the session. Both of you contribute to this.
- Homework review. You discuss what you practiced between sessions, what worked, and what felt difficult.
- Skills work. The core of the session. You apply a specific technique, such as cognitive restructuring or an exposure exercise, to a real problem.
- Summary and new homework. You recap what you learned and agree on what to practice before the next session.
That structure repeats across all 12 to 16 sessions. Early sessions tend to focus on psychoeducation, meaning understanding the CBT model and how it applies to your situation. Later sessions focus on applying skills independently.
One thing many patients do not expect: early discomfort is common. When you start examining distorted thoughts, it can feel unsettling. Clinicians view that discomfort as a sign of engagement, not a sign that therapy is making things worse. Sitting with that discomfort is part of the process.
Pro Tip: Tell your therapist when something feels too hard or not relevant. CBT is collaborative. Adjusting the approach is normal and expected, not a failure.
Honesty matters more than you might think. The more accurately you describe your thoughts and behaviors, the more precisely your therapist can help. Presenting a polished version of yourself slows the work down.
Key Takeaways
CBT is the most evidence-supported psychotherapy available for anxiety, depression, PTSD, and OCD, and its effectiveness depends directly on active patient participation and consistent homework practice.
| Point | Details |
|---|---|
| CBT is structured and time-limited | Most programs run 12–16 weekly sessions of about 50 minutes each. |
| Cognitive restructuring is the core skill | You test the accuracy of distorted thoughts, not replace them with positivity. |
| Homework drives real progress | Between-session practice is where lasting change is built, not just in the room. |
| Evidence is strong across conditions | JAMA Psychiatry meta-analyses confirm large effect sizes for depression, anxiety, PTSD, and OCD. |
| CBT works best combined with medication for severe cases | Combining both treatments outperforms either alone for moderate-to-severe depression and panic disorder. |
What I have learned from watching CBT work and fall short
CBT is genuinely powerful. We see that in our work with patients across Allen, Frisco, McKinney, and Plano. But I want to be honest about something most articles skip: CBT is not passive. It asks a lot of you.
The patients who get the most from it are not necessarily the ones with the mildest symptoms. They are the ones who show up to sessions prepared, complete their thought records between appointments, and are willing to sit with discomfort when a technique feels hard. That willingness is the variable that matters most.
Where I have seen CBT fall short is with patients who expect the therapist to do the work for them. CBT is collaborative, not prescriptive. Your therapist is a guide, not someone who fixes your thinking for you. That distinction changes everything about how you engage with the process.
I have also seen patients give up right when things start to get productive. That early spike in anxiety during exposure work or cognitive restructuring is not a red flag. It is a signal that the therapy is touching something real. Pushing through that phase, with support, is where the gains live.
For complex trauma or deep-seated attachment difficulties, CBT alone may not be enough. Longer-term approaches can be necessary for durable results. Knowing that upfront helps you set realistic expectations and avoid feeling like you failed if CBT needs to be part of a broader plan rather than the whole plan.
— Felix
Mental health care in North Dallas: what comes next
If you are considering CBT or want to understand whether it fits your situation, a conversation with a licensed psychiatrist is the right first step. At Nortexpsychiatry, we work with patients across Allen, Frisco, McKinney, and Plano to build care plans that match the severity and nature of what they are dealing with. For some patients, CBT alone is the right path. For others, medication management alongside therapy produces better outcomes. We also offer a self-assessment tool if you want a structured starting point before scheduling a consultation. Both in-person and telehealth appointments are available.
FAQ
What is the main goal of cognitive behavioral therapy?
CBT aims to reduce psychological distress by helping you identify and change inaccurate or unhelpful thought patterns that drive negative emotions and behaviors. The goal is lasting skill-building, not just symptom relief during sessions.
How long does cognitive behavioral therapy take to work?
Most patients complete a standard program of 12 to 16 weekly sessions. Some notice meaningful improvement within the first 6 to 8 sessions, particularly for anxiety and depression.
Is cognitive behavioral therapy effective for anxiety?
Yes. Meta-analyses confirm CBT produces large effect sizes for generalized anxiety disorder, panic disorder, and social anxiety, and very large effect sizes for specific phobias and PTSD. It is considered a first-line treatment for most anxiety conditions.
Can CBT be done online or by telehealth?
CBT is well-suited to telehealth delivery. Research supports that video-based CBT produces outcomes comparable to in-person sessions for most conditions, including anxiety and depression.
Do I need medication alongside CBT?
Not always. For mild to moderate symptoms, CBT alone is often sufficient. For moderate-to-severe depression or panic disorder, combining CBT with medication consistently outperforms either treatment on its own.



