
Integrated mental health is the systematic coordination of mental health, substance use, and primary care services into a single, unified treatment model. Rather than sending you to three separate providers who never speak to each other, this approach places your care under one coordinated team. The American Psychological Association, the Agency for Healthcare Research and Quality (AHRQ), and the Milbank Memorial Fund have all contributed to defining and refining this model. The core idea is straightforward: your mind and body are not separate problems, so your care should not be either.
What is integrated mental health and how does it work?
Integrated mental health is defined as the systematic coordination of mental health, substance use, and primary care services in a unified care delivery model. This means your psychiatrist, therapist, and primary care doctor are not working in silos. They share information, align on goals, and adjust your treatment together.
The operational backbone of this model is a shared electronic health record. Providers update treatment plans in real time, so your psychiatrist knows what your primary care doctor prescribed last week, and vice versa. That real-time alignment prevents conflicting advice and redundant testing.

Team-based care is the defining feature. A typical integrated team includes a primary care physician, a behavioral health specialist such as a psychologist or licensed counselor, a care manager, and a consulting psychiatrist. Each member works at the top of their licensure. A care manager, for example, tracks your progress and flags concerns between appointments. The psychiatrist consults on complex medication decisions without necessarily meeting you directly every session.
Task-sharing and communication protocols allow specialists to operate at their highest competency while staying aligned. This is not about merging roles. It is about structured collaboration.
- Shared electronic health records updated across all providers in real time
- Unified treatment plans that address mental health, physical symptoms, and life stressors together
- Regular team communication through case reviews, warm handoffs, and care manager check-ins
- Task-sharing so each provider focuses on what they do best
Pro Tip: Ask your care team directly: “Do you share records with my other providers?” If the answer is no, you may be in a co-located model rather than a fully integrated one. The distinction matters for your outcomes.
What are the benefits of integrated mental health care?
The benefits of integrated mental health are measurable and well-documented. Patients in integrated care experience faster symptom relief, better treatment adherence, and higher overall satisfaction compared to those in traditional siloed models.
Here is what the evidence shows:
-
Faster symptom relief. Patients in integrated care often see improvement within weeks rather than the months typical of separate, sequential care. Coordinated interventions mean problems are caught and addressed earlier.
-
Whole-person wellness. Integrated care prioritizes quality of life improvements over service volume. Providers are oriented toward your outcomes, not just the number of appointments you attend.
-
Fewer conflicting treatments. When your psychiatrist and primary care doctor share a treatment plan, you are far less likely to receive medications that interact badly or advice that contradicts itself.
-
Higher treatment adherence. A 2021 review found that integrated care models effectively reduce mental health burdens, particularly through task-sharing and telemedicine. Patients stay engaged longer because the system meets them where they are.
-
Reduced burden on primary care. APA experts note that integrated care relieves primary care physicians from being the sole gatekeepers of mental health. That shift improves clinical decision-making for everyone on your team.
The contrast with traditional care is stark. In a traditional model, you might wait weeks for a psychiatry referral, then more weeks for a therapy appointment, while your primary care doctor remains unaware of either. Integrated care compresses that timeline and keeps every provider informed.
What are the main models for delivering integrated mental health?
The Milbank Memorial Fund outlined eight behavioral health integration models, ranging from minimal coordination to full clinical integration. Understanding these models helps you recognize what level of care you are actually receiving.
The two most widely used frameworks are the Collaborative Care Model (CoCM) and the Primary Care Behavioral Health (PCBH) model. They differ in structure, team roles, and the patient populations they serve best.
| Model | Structure | Best suited for |
|---|---|---|
| Collaborative Care Model (CoCM) | Primary care provider, care manager, consulting psychiatrist | Moderate to severe depression, anxiety, PTSD |
| Primary Care Behavioral Health (PCBH) | Embedded behavioral health consultant in primary care | Broad population, mild to moderate concerns |
| Co-location | Separate providers sharing a physical space | Patients needing referrals with warm handoffs |
| Full clinical integration | Unified team, shared records, single treatment plan | Complex, multi-diagnosis patients |
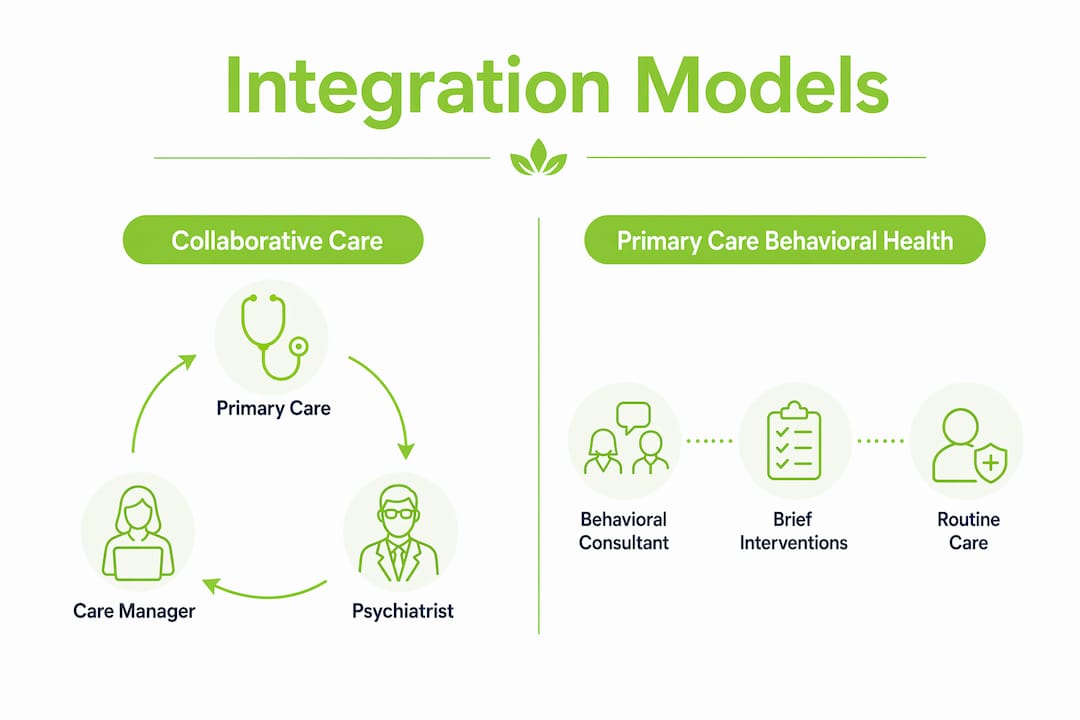
In the Collaborative Care Model, patients with severe mental illness receive care from primary care providers and case managers, supported remotely by consulting psychiatrists. The psychiatrist may never meet you directly. Instead, they review your case data and advise the team. This model supports medication management and psychoeducation at scale.
Co-location is often mistaken for full integration. Two providers sharing a building is not the same as two providers sharing a treatment plan. True integration is defined by shared protocols and communication, not physical proximity.
The severity of your mental health condition influences which model fits best. Mild anxiety managed alongside a routine physical fits the PCBH model well. Treatment-resistant depression or co-occurring substance use disorders call for the deeper coordination of full clinical integration or CoCM.
How does integrated care address physical health and lifestyle?
Mental health does not exist separately from your body. Lifestyle factors like sleep deprivation and nutritional deficiencies are treated actively within integrated mental health, and they influence recovery outcomes significantly. This is one of the clearest distinctions from traditional psychiatric care, where a therapist might never ask about your sleep schedule or diet.
In an integrated model, your treatment plan includes physical health data. Blood work, sleep patterns, exercise habits, and stress levels all feed into how your team adjusts your care. A psychiatrist might notice that your persistent fatigue is tied to a thyroid issue your primary care doctor is already tracking. That connection gets made because the records are shared.
Key lifestyle factors addressed in integrated care:
- Sleep quality as a direct variable in mood regulation and medication response
- Nutrition and metabolic health linked to depression and anxiety severity
- Stress management techniques such as mindfulness-based cognitive therapy (MBCT) coordinated with medication
- Physical activity recommended as part of the treatment plan, not just general wellness advice
Shared decision-making is central to this process. You are not handed a plan. You help build it. Your providers explain the reasoning behind each recommendation, and you give feedback on what is working. That back-and-forth is built into the model.
Pro Tip: When you start with an integrated care team, bring a written summary of your sleep patterns, current medications, and any physical symptoms you have noticed. This gives your team a faster, clearer starting point than a standard intake form.
The role of lifestyle in mental health is not a soft add-on in integrated care. It is treated as clinical data. That shift in framing changes what your providers ask, what they track, and how they measure your progress.
Continuous evaluation is another feature that sets integrated care apart. Your team does not wait for a crisis to reassess your plan. Regular check-ins, outcome measures, and care manager follow-ups keep your treatment current. If something stops working, the team adjusts quickly because they are already in communication.
Key takeaways
Integrated mental health is the most effective care model for treating the whole person because it coordinates mental, physical, and lifestyle factors under one unified team with shared records and aligned goals.
| Point | Details |
|---|---|
| Core definition | Integrated mental health coordinates mental health, substance use, and primary care into one unified model. |
| How it works | Shared electronic records and task-sharing keep all providers aligned on a single treatment plan. |
| Key benefit | Patients experience faster symptom relief and higher treatment adherence than in traditional siloed care. |
| Main models | The Collaborative Care Model and Primary Care Behavioral Health model serve different severity levels and settings. |
| Lifestyle inclusion | Sleep, nutrition, and stress are treated as clinical variables, not afterthoughts, within integrated care plans. |
What I have learned about integrated care after years in practice
The concept sounds clean on paper. In practice, it requires something most healthcare systems are not naturally built for: consistent, humble communication between providers who were trained to work independently.
What I have noticed over time is that patients often arrive expecting integration to mean one provider who does everything. That is not what it is. The value is in the coordination, not the consolidation. When a care manager calls a patient three days after a medication change to check in, that is integrated care doing its job. When a primary care doctor flags a new blood pressure reading to the psychiatrist before the next appointment, that is the model working as intended.
The misconception I hear most often is that integrated care is only for people with severe or complex conditions. That is not accurate. The early action in mental health that integrated models enable is precisely what prevents mild concerns from becoming serious ones. The structure supports everyone, not just those in crisis.
What I would tell anyone choosing between care models: ask how your providers communicate with each other. Ask who holds your unified treatment plan. Ask what happens between appointments. Those three questions will tell you more about the quality of integration than any brochure will.
Recovery is not a straight line. Integrated care does not promise otherwise. What it does promise is that when you hit a rough patch, your whole team knows about it at the same time, and they respond together.
— Felix
How Nortexpsychiatry supports coordinated mental health care
At Nortexpsychiatry, we work with patients across Allen, Frisco, McKinney, and Plano using the same principles that define integrated mental health: coordinated care, shared decision-making, and treatment plans that account for the whole person. Our services include psychiatric evaluations, medication management, and advanced options like TMS therapy for patients who have not responded to standard treatments. You can review a side-by-side treatment comparison to understand which approach fits your situation. For a structured starting point, our step-by-step care guide walks you through what coordinated psychiatric care looks like in practice. Both in-person and telehealth appointments are available.
FAQ
What is the definition of integrated mental health?
Integrated mental health is the systematic coordination of mental health, substance use, and primary care services within a single, unified treatment model. It replaces fragmented, siloed care with team-based approaches that treat the whole person.
How does integrated mental health differ from traditional care?
Traditional care routes patients to separate providers who rarely communicate. Integrated care uses shared records, unified treatment plans, and regular team communication to keep all providers aligned on the same goals.
What is the Collaborative Care Model in integrated mental health?
The Collaborative Care Model (CoCM) places a care manager and consulting psychiatrist alongside a primary care provider to support patients with moderate to severe mental health conditions, often without requiring direct psychiatrist-patient meetings.
Who benefits most from integrated mental health services?
Integrated mental health services benefit a broad range of patients, from those managing mild anxiety alongside physical health concerns to those with complex, co-occurring conditions requiring coordinated medication and therapy adjustments.
Is co-location the same as integrated mental health?
Co-location means providers share a physical space but does not guarantee shared records or unified treatment plans. True integration is defined by coordinated communication and aligned care strategies, not proximity.



